What is a hernia?
Hernia Basics
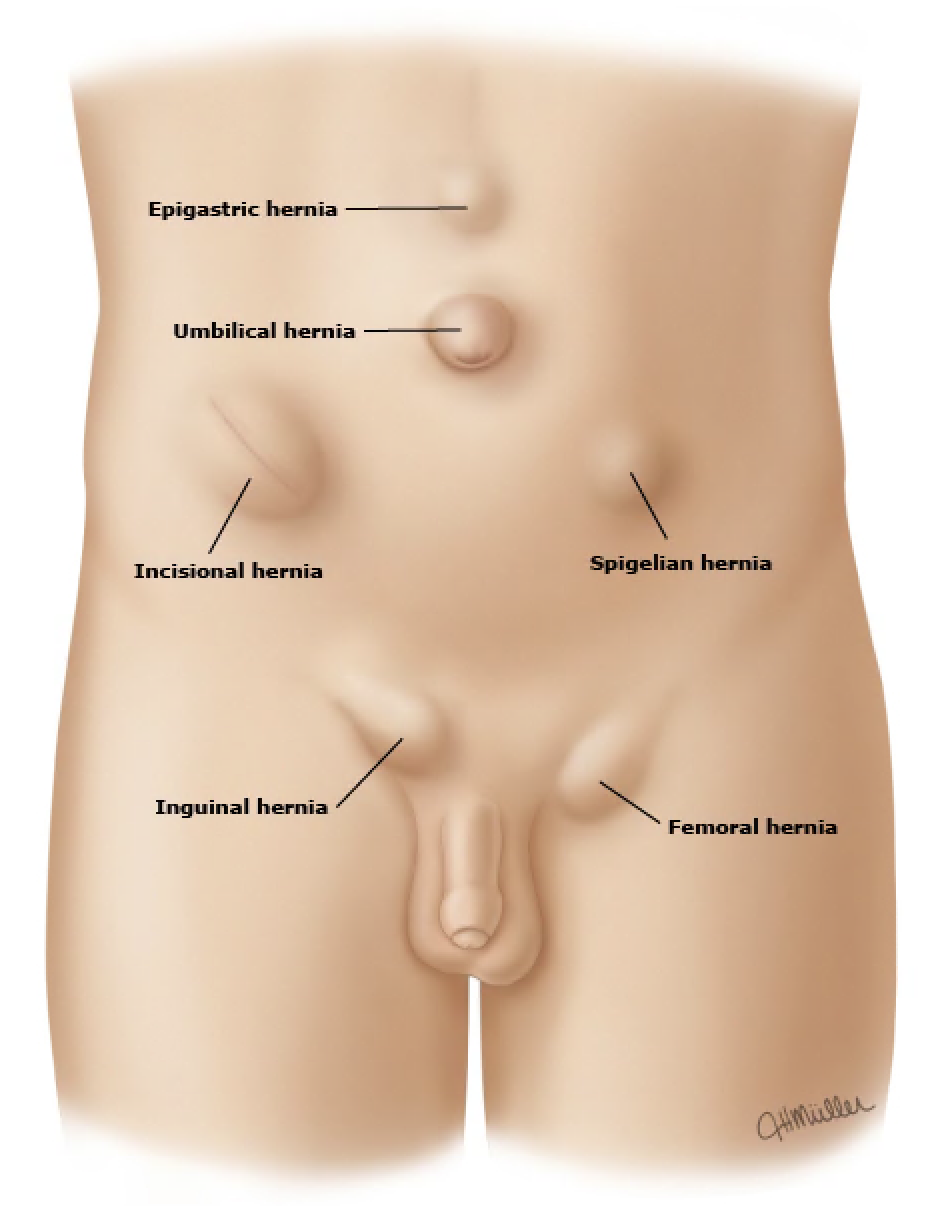
A hernia is a tear in the muscle of the abdominal wall. Over time they grow in size and the contents of your abdomen (fat or intestine) can begin to protrude through these holes. They can become painful if the contents become stuck in the hole. Hernias do not get better on their own. The only way to fix these is through surgery. Hernias can occur spontaneously or through prior surgical incisions. Men are more prone to groin hernias (Inguinal hernias) than women, however they can occur in anyone.
Hernia contents can often be manually pushed back into the abdomen but will usually pop back out. If the contents become stuck and the hernia becomes very painful this can be a surgical emergency and will need to be fixed as soon as possible. Most hernias can be fixed electively and do not require a hospital stay.
Laparoscopic INguinal/Femoral Hernia Repair
Using a minimally invasive approach I am able to fix these groin hernias through three small incisions, the largest incision is about an inch in length and the other two are about half an inch. Using this approach helps you get back to your regular life and activity with minimal down time. Typically patients can resume all activity within a couple of days. The contents and hernia sac are reduced from their attachments and the area is reinforced with a mesh that acts as a scaffold for healthy tissue to build a barrier against any recurrence of the hernia.


Ventral Hernias
Ventral hernia is an overall term used for any hernia of the abdominal wall. It includes incisional, umbilical, supra umbilical, and spigelian hernias. The overall approach is basically the same regardless of the subtype. The contents are removed from the hernia and then the defect is closed from inside the abdomen. A mesh is placed over the repair to enhance the strength of the abdominal wall and prevent the hernia from coming back. Usually three incisions are used, one is about an inch and all the other incisions are about half an inch. Depending on the complexity of the hernia, two additional small incisions are sometimes needed
Depending on the size of the hernia a minimally invasive approach is not always possible. Very large hernias require an open tactic, information on this is listed below.
Abdominal wall reconstruction

Sometimes hernias can become so large that a minimally invasive approach is not enough. In these cases a complex abdominal wall reconstruction is performed. The abdominal wall is like a sandwich of layers. There are 4 sets of muscle groups enveloped in connective tissue called fascia that make up the abdominal wall. A reconstruction of the wall with large (usually greater than 8 cm) holes requires us to separate the layers in order to have enough tissue to adequately close up the defects. There are some exciting new techniques being developed to perform this with small incisions, however currently this needs a large incision down the middle of the abdomen for adequate repair. This operation usually requires a day or two in the hospital while you recover.
A word about meshes
There is a lot of misinformation out there about medical meshes. The truth is that there are some types of mesh that has caused problems, but they typically are related to gynecological procedures in the pelvis. Some are related to outdated technology in some of the older versions of mesh. If I thought mesh was a problem I wouldn’t use it. The fact is, using mesh reduces the chance of recurrence significantly. Inguinal repair with a mesh reduces recurrence down to about 1% from about 10% without a mesh. Ventral hernia recurrence rate with a mesh ranges from 1-3% with mesh and almost 20% without a mesh. If you want to investigate further on your own, I prefer to use a mesh called Synecor, made by Gore. This is a free plug for them, I have no financial interest in that company or their line of products, but I think its easy to work with and have had great results using it. If you do have concerns I am happy to discuss the topic when you see me in the office!